Getting a Handle on the COVID-19 Pandemic
By Geoffrey C. Kabat
“Geoffrey Kabat’s vital, wide-ranging book cannot have arrived at a more fortuitous time. . . Everyone should read his analysis—at once clear-eyed, thoughtful, and beautifully written—to understand the nature of risk. I cannot overstate the importance of this book.”
~Siddhartha Mukherjee, author of The Emperor of All Maladies
Geoffrey Kabat is a cancer epidemiologist and author of Getting Risk Right: Understanding the Science of Elusive Health Risks, which is now available in paperback. Kabat joins us today to explain the COVID-19 pandemic, from its outset to what lies ahead.
• • • • • •
The first case of what we now know to be COVID-19 was diagnosed on November 17, 2019, in Hubei province in China. Six weeks later, on December 31, China reported a cluster of cases of pneumonia in the city of Wuhan, the capital of Hubei province. One week later, Chinese health authorities confirmed that this outbreak was associated with a novel coronavirus, SARS-CoV-2.
Wuhan is a provincial hub in central China with a population of 11 million. The virus was carried by travelers from Wuhan to other cities in China, Hong Kong, South Korea, Taiwan, and elsewhere in Asia and beyond, with major outbreaks occurring relatively early in Iran and Italy. The virus is now present in more than 200 countries.
The first case of infection in the United States was reported on January 20, 2020, in a nursing home outside of Seattle. As of today, the virus has spread throughout the United States, with major outbreaks in New York City, Los Angeles, Seattle, Detroit, Atlanta, St. Louis, Denver, Houston, Dallas, Washington, DC, Baltimore, and Chicago and across New Jersey, Florida, and Louisiana. As of April 6, the number of confirmed cases is approaching 300,000 and increasing hourly. The United States has by far the largest number of confirmed cases of any country, followed by Italy. New York City is hardest hit.
“The United States has by far the largest number of confirmed cases of any country, followed by Italy. New York City is hardest hit.”
In order to make sense of the constantly increasing numbers and understand how we arrived at this point and where we are headed, it helps to examine what we know so far about the COVID-19 pandemic in light of the core principles and concepts used in the study of infectious diseases and epidemiology generally.
Epidemiologists are taught to think about any disease outbreak in terms of person, place, agent (in this case, the virus), and time. It is the interaction of all of these factors that determines the extent of an outbreak. Understanding the nature of the interaction of the agent, SARS-CoV-2, with its environment holds the key to controlling an outbreak.
The Agent
The SARS-CoV-2 virus is a new infection in humans, and there is a lot we don’t know about it. But we quickly learned several basic facts.
Infected people are capable of spreading the virus for several days before the onset of symptoms, and some carriers may be totally asymptomatic. (These have been dubbed “super-spreaders.”) On average, without any intervention, a carrier will infect 2.0–2.5 people. This is called the reproductive number or R0. For comparison, the seasonal flu has an R0 of 1.3. As long as the R0 is greater than 1, the virus will continue to spread.
“Infected people are capable of spreading the virus for several days before the onset of symptoms, and some carriers may be totally asymptomatic.”
SARS-CoV-2 has an incubation period of 1–14 days, compared to 1–4 days for the seasonal flu. Because of the long incubation period, infected people can spread the virus for a substantial period of time. Another consequence of the long incubation period is that the number of diagnosed cases represent only a fraction of those who are infected with the virus. This means that when we use the number of diagnosed cases as an indicator, we are several weeks behind where the infection actually is.
In addition, it should be noted that although the highest hospitalization rates and death rates are seen in older people and those with preexisting conditions, the infection can do serious damage to young people’s lungs and cause death. We have known since January from the information coming out of Wuhan that this is a very destructive pathogen, possibly because it infects both the upper and lower respiratory tracts.
Time: Exponential Growth
From January 21 to March 1, the number of cases in the United States grew but had only reached the double digits. However, the curve soon started to bend upward and became progressively steeper. In 27 days (from March 2 to March 29) the number of cases ballooned from 118 to 161,800—over a thousand-fold increase. This is exponential growth. For every day that is lost, you are higher up on an ever-steepening epidemic curve.
The overall statistics for the United States are reflected in cities and towns throughout the country, with rates of growth varying depending on when the outbreak was seeded, the local characteristics (e.g., population density), personal behavior, and state and local policies.
Tamping Down the Spread of the Virus
To bend the epidemic curve downward, you need to reduce the R0. Anything that reduces the opportunities for infection will reduce the R0. This is the logic behind the guidelines calling for “social distancing,” practicing careful hygiene, isolating infectious individuals, and “lockdowns” (closing schools and places of work). In addition, steps, such as those taken in mid-March in New York City, to close museums, theaters, and restaurants and cancel meetings further limited opportunities for transmission.
“We now have plenty of evidence that the time to enact restrictions on contact is as soon as the first cases are detected, before spread pushes the curve upward.”
Roughly, 90 percent of the United States is on some form of lockdown as a result of haphazard decisions by governors and mayors. Some states have either partial restrictions or no restrictions. However, we now have plenty of evidence that the time to enact restrictions on contact is as soon as the first cases are detected, before spread pushes the curve upward. Clearly, given the tendency toward exponential growth, the earlier these kinds of actions are taken and the more comprehensive they are, the lower on the curve the virus will be slowed or stopped.
Evidence from multiple countries shows that efforts to reduce the spread of infection are able to flatten the epidemic curve. However, there is the likelihood that a second wave of infection will occur when restrictions are relaxed and carriers of the virus seed new outbreaks. This has occurred in China and is happening in Singapore after both countries appeared to have quashed the pandemic. Until an effective vaccine becomes available, localities will have to be on the alert for new infections and be ready to reintroduce control measures.
Need for Testing
Owing to the lag between infection and the appearance of symptoms and because new sources of infection are seeded and develop for weeks before being recognized, widespread testing is crucial. The test that detects the virus can be used in two different ways. First, clinical testing of those with symptoms and their contacts can be used to confirm the presence of the coronavirus. This makes it possible to isolate patients during the infectious period and trace their contacts.
Second, we urgently need to know the extent of infection in the general population. For this, we need testing of a random sample of the population. This type of survey should be carried out now. Estimates of the death rate from COVID-19 range from 1 to 3.4 percent.
However, because testing is badly skewed toward those who are sick, the case fatality rate (the number of deaths among those who are infected/the total number infected with the virus) could be seriously overestimated. There are indications, in fact, that the case-fatality rate is below 1.0 pecent. This means that the number-one priority should be conducting a survey of a random sample of the population.
“There is another kind of testing that will be essential when the first wave of the outbreak has been brought under control.”
There is another kind of testing that will be essential when the first wave of the outbreak has been brought under control. This is serological testing of representative samples of the population in order to determine who has antibodies to the virus—a sign that a person has been infected and has successfully mounted an immune response. Without this kind of testing, we are in the dark about what proportion of the population has had the infection and survived.
Furthermore, those who have recovered from the virus are expected to have at least short-term immunity to the virus (lasting several years) and could, thus, be able to return to work and move freely without endangering those who are still susceptible.
Murky Modeling
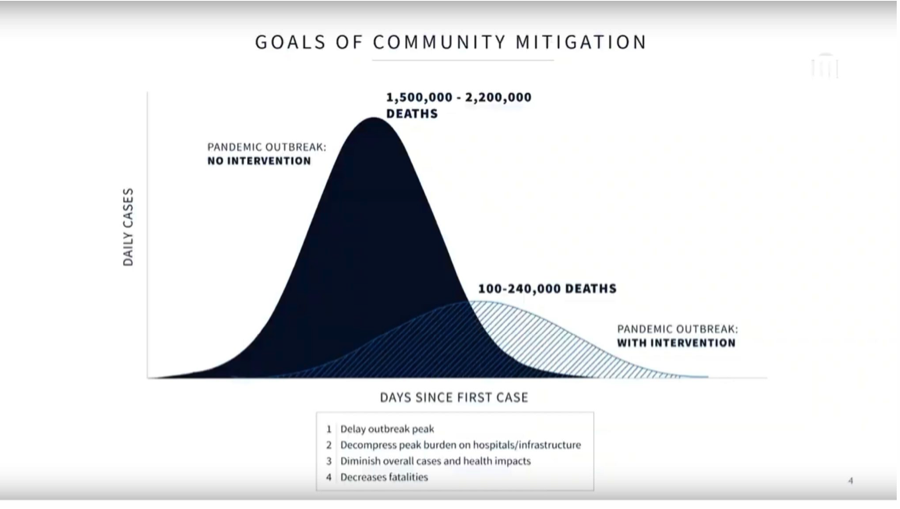
On March 3 at the White House COVID-19 briefing, government scientists cited figures suggesting that the coronavirus could kill between 100,000 and 240,000 Americans under the best-case scenario (adherence to social-distancing measures and a nationwide lockdown). Within two days, the numbers were already being revised upward because of state intransigence on closings. The projections indicated that without stay-at-home restrictions on people’s movements the toll could be as high as 2.2 million.
The White House did not specify the time period over which these deaths were to take place, and modelers at universities were mystified by what they believe are lowball projections. Asked about the models, Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, commented that there are too many variables at play in the pandemic to make the models reliable: “I’ve looked at all the models. I’ve spent a lot of time on the models. They don’t tell you anything. You can’t really rely upon models.”
China’s Deception
Any account of the response to the COVID-19 outbreak has to start with the fact that, as late as mid-January, China, with the full-throated agreement of the WHO, argued that there was no evidence of person-to-person transmission. Local government officials in Wuhan were slow to report news of the outbreak to Beijing and detained doctors and journalists who tried to notify the world of the growing outbreak.
During the month of January, even as State Department and CDC officials were warning of an impending global crisis, more than 300,000 travelers came to the United States from China. On January 24, the CDC confirmed two cases of the novel coronavirus in the United States from people who had returned from Wuhan. U.S. intelligence agencies warned that China was concealing the extent of the outbreak and relayed those warnings directly to President Trump. But he insisted that China was being candid and had the virus under control. Secretary of Health and Human Services Alex Azar, Center for Disease Control head Robert Redfield, and Anthony Fauci all recommended a travel ban, but Trump rebuffed them.
“U.S. intelligence agencies warned that China was concealing the extent of the outbreak and relayed those warnings directly to President Trump.”
Finally, on January 31, at the insistent urging of HHS and lobbying by Senator Tom Cotton of Arkansas, and after numerous airlines had suspended service to China, President Trump stopped the few remaining flights to the United States from China. It was only a partial shutdown; the policy prohibited non-U.S. citizens, other than the immediate family of U.S. citizens and permanent residents, who had traveled to China within the previous two weeks from entering the United States.
The partial ban came late, but it was an important step in slowing down the spread of the virus. However, it was accompanied by no other measures.
Aftermath
As if there were not enough variables involved in the viral pandemic and the human response to it, our handling of the pandemic has been marked by bureaucratic bungling, politicization of the issue, and a failure to learn from the experience of other countries. The outbreak has sparked an epidemic of misinformation about the virus that has fed on distrust of experts. A favorite meme, perpetrated most aggressively by the president and FOX News as recently as mid-March, has been to trivialize COVID-19 by likening it to the seasonal flu even though it is more transmissible and has a much higher hospitalization rate than seasonal flu.
Rather than taking charge of the crisis, from the first, President Trump has consistently downplayed the seriousness of the outbreak, delivered false messages, and shown little evidence that he has any real grasp of or interest in what is happening, leading to many video montages of his repeated inaccurate misstatements. Instead, he has constantly betrayed his preoccupation with the stock market, the coming election, and his poll numbers. This has left us without a leader who is capable of showing empathy for people and an understanding of the impact of the crisis on their lives.
“As if there were not enough variables involved in the viral pandemic and the human response to it, our handling of the pandemic has been marked by bureaucratic bungling, politicization of the issue, and a failure to learn from the experience of other countries.”
The Obama administration had prepared an extensive report predicting a pandemic worse than the crippling 1918 Spanish flu was possible. Before Trump’s inauguration, incoming officials were told such a pandemic would likely lead to shortages of ventilators and that a coordinated national response would be “paramount,” according to documents obtained by Politico.
Infectious-disease experts have warned for decades that sooner or later a new virus would jump from an animal host to humans or that a known virus would mutate, acquiring a high enough transmissibility and lethality to become a pandemic that could kill millions of people worldwide. The Johns Hopkins Center for Health Security gathered public-health experts, business leaders, and U.S. government officials in 2018 and 2019 for simulations of the devastating humanitarian, political, social, and economic consequences of fictional novel coronaviruses that left tens of millions dead around the world.
The warnings went unheeded, and under Trump’s direction and consistent with his goal of gutting government agencies, whose purpose and value his advisors and appointees were inimical to, in 2018 the White House ordered that the pandemic-preparedness group on the National Security Council be disbanded. When asked about this, Trump professed to have no knowledge of the change.
“Infectious-disease experts have warned for decades that sooner or later a new virus would jump from an animal host to humans or that a known virus would mutate, acquiring a high enough transmissibility and lethality to become a pandemic that could kill millions of people worldwide.”
On other fronts as well, there have been depressing failures to do things that advanced countries in Asia and some in Europe have been able to deploy on the needed scale. Over the weekend of January 11–12, the Chinese authorities had shared the full genome of the coronavirus, as detected in samples taken from the first patients. And the WHO and countries like Taiwan and South Korea quickly developed tests to detect the virus. However, here the development of a test was bungled by the CDC and the FDA.
Testing of people with symptoms is still not available in many places, and it can take more than a week to get results—in spite of what the president repeatedly insists. This means that for more than two months, many people infected with the virus have not been identified, and their contacts have not been traced, leading to further spread.
In the United States, stocks of personal protective equipment (PPE) and ventilators are woefully inadequate, and hospitals and states are competing on the open market for these indispensable products, both among themselves and with FEMA. Reports from hospitals in different cities tell of medical workers having to reuse the same mask throughout the day, rather than changing it after each patient contact.
A report in the New York Times on April 2 revealed that the strategic ventilator stockpile is depleted, that the maintenance contract for a store of roughly 10,000 ventilators held in reserve by the federal government was allowed to lapse, and that a significant proportion of the ventilators do not work.
“In the United States, stocks of personal protective equipment (PPE) and ventilators are woefully inadequate, and hospitals and states are competing on the open market for these indispensable products, both among themselves and with FEMA”
Even with all of the failures and lost time, it looks like a majority of the country is finally coming around to grasping the need to comply with measures to control the virus. Places that have been slow to embrace lockdowns will likely be spurred to greater compliance as more cases begin to appear in their localities and after witnessing the spikes from New York City to rural Louisiana.
What Lies Ahead
Today we face a crisis of staggering proportions affecting every person, particularly health-care workers, as well as the economy. But because there are so many unknowns about the novel virus, no one can say how the next months and year will play out. We desperately need to learn the extent of infection in the general population by undertaking testing of a random sample. Once this is accomplished, a second survey of a random sample of the population for antibodies to the virus will provide crucial information enabling decisions about a return to normal life.
There are a number of other crucial questions that need answers:
-
- What percentage of carriers is asymptomatic?
- How many people are dying with the virus, rather than from the virus, i.e., people who would have died within a short period time even without infection?
- What proportion of deaths had one or more medical conditions?
Until this crucial information is available, all we can do is follow the prescriptions of scientists who have devoted their careers to the study of viruses and outbreaks and learn from the experience of other countries that are ahead of us in confronting the infection. Private and public laboratories around the world are racing to develop and test treatments and vaccines. While we wait for these efforts to yield tangible results, we will all need to do everything we can to avoid acquiring the virus and adding to the burden on the medical system. One thing the virus makes clear is that we are all in this together.
In the longer perspective, we should remember that experts have been warning for decades of a pandemic ignited by new, lethal, and highly transmissible virus. SARS-CoV-2 is not the worst pathogen that was envisaged, but it is bad enough. If these warnings had been heeded and we had prepared better for a coming pandemic, we would not be contemplating the distressing failures on so many fronts and their tragic consequences.